A Guide to Early ACL Rehabilitation
By Julie Hubbard
Whenever an athlete pivots or jumps awkwardly and hears a “pop” in her knee, the first thought is usually, "Oh {bleep}." The second thought is, "I hope it's not my ACL." And the third usually goes something like, "I can't possibly sit out for six whole months."
Early ACL rehabilitation is the start of what can be a long journey ahead. As you might know, ACL injuries can take anywhere from six to nine months and sometimes even up to twelve months of rehabilitation before an athlete may find herself back on the field. Sustaining an ACL injury is not only a physical but an emotional blow where an athlete's entire world is flipped upside down.

By my fourth ACL injury, I really couldn't wrap my head around enduring rehabilitation again. I remember waiting in pre-op staring at my heart rate jumping on the monitors, and watching the saline drip into my IV. I distinctly remember the feeling of dread that grew more and more with each second that ticked down towards my surgery time.
My only comfort lay in the fact that I knew exactly what would happen next. I'd been in this situation multiple times before. I knew I would wake up in the recovery room, my leg would be completely numb, and my knee would already be braced up. As a 4x member of the ACL club and now a sports physical therapist, I knew exactly what the next few months had in store for me.
Today's post will focus on early ACL rehabilitation - those first four to eight weeks after waking up in the recovery room. Maybe this post applies to you, or perhaps you know someone about to go through the process. Knowing "what comes next" can be extremely helpful in calming those nerves, so please feel free to hit the share button (teamwork does make the dream work, after all).
What Expect During Early ACL Rehabilitation
It's important to realize that everyone's rehabilitation will be slightly different. Different surgeons advocate for different approaches and different post-operative protocols. Some may require you wear a knee immobilizer up to 6-weeks post-op, while others may not even brace you. Rehab will change slightly if other ligaments, bony, or cartilaginous structures of the knee are also repaired, so please remember this is not a "one-size-fits-all" situation. There are, however, many fundamental similarities in rehabilitating an anterior cruciate ligament, and I will lay them out below.
Pain Management
Once you return home from the hospital, it will be imperative to let the knee calm down. I know that we, athletes, like to hit the ground running so-to-speak, but doing too much, too fast can slow down your recovery. Step one is to manage your pain appropriately. Only use medication in consultation with your physician, and remember that getting on a regiment and staying on top of the pain before it escalates, can be a huge game-changer. Ice and cryocuff machines can also be excellent alternatives to the opioid medications frequently prescribed post-operatively.
Swelling Reduction
After pain management comes swelling reduction. An ACL reconstruction is a traumatic experience. The knee will inevitably swell up, and you will have a moderate amount of joint effusion. Bruising is also completely normal. Remember to keep your leg elevated and compressed in an ACE wrap bandage. Propping your leg up on a pillow above the level of your heart and performing simple ankle pumps can also help facilitate venous return back to the heart.

Quadriceps Activation
During this stage of rehab, "quad sets" will become your new best friend. Quadriceps setting is when a patient squeezes the anterior thigh muscles as much as possible to straighten the knee. I often tell my patients to do up to 1,000 per day because the sooner they regain neuromuscular control of their quads, the quicker they can progress through rehab.
Many patients encounter a strange phenomenon during this stage, where they cannot physically activate their thigh muscles. Marked quadriceps weakness is typically observed following injury, surgery, or pathology affecting the knee joint when significant swelling is present. This is partly due to ongoing neural inhibition that prevents the central nervous system from fully activating the quadriceps, a process known as arthrogenic muscle inhibition, or AMI.
If you are having a hard time turning on your quad muscles, don't panic! A study by Sonnery-Cottet et al. looked at different therapeutic interventions used to treat AMI in post-op ACL patients. After reviewing over 780 studies, they found moderate-quality evidence supporting the use of cryotherapy and exercise to decrease AMI. While many physical therapists elect to use Russian Stim or Neuromuscular Electrical Stimulation (NMES) to "wake up" the quad muscles, these researchers only found low-quality evidence supporting the use of such modalities. So, what does this mean for you? Ice can not only decrease pain but can also increase muscle activation. So lose the stim pads and pull out the frozen peas!

Quadriceps Setting
Knee Extension Range-of-Motion
Maintaining full knee extension (or hyperextension) is another major goal of the initial recovery phase. For this reason, many doctors advocate for maintaining the knee brace locked out at zero degrees to prevent the knee from bending for prolonged periods of time. Once lost, regaining flexion (or knee bend) is much easier than regaining knee extension. Losing terminal knee extension can lead to many consequences, including anterior knee pain, altered movement mechanics, and difficulty walking. But don't worry! There are many ways to prevent this from happening. Your physical therapist will give you a bunch of stretches for the calf and hamstring musculature to ensure that you can fully extend your knee. I've included a few helpful pictures below:

Calf Stretching
Hamstring Stretching
Long Duration Stretches
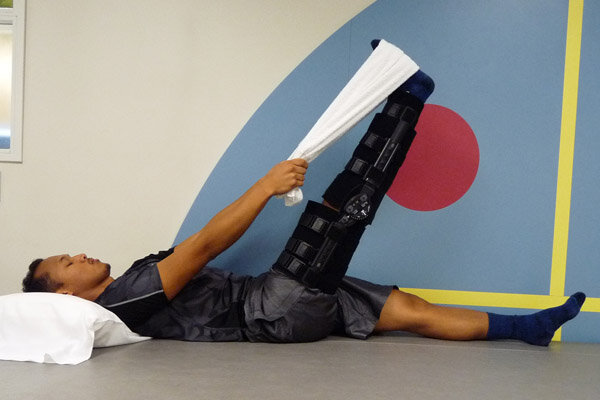
Another useful trick to help you cruise past early post-op rehab is something called the low-load, long-duration stretch (LLLD stretch). This is basically a gentle stretch held for a prolonged period of time and can be useful in patients who have elevated levels of pain or discomfort. You can do this by propping your heel up on a towel or foam roll and by then placing a 5-10 pound weight on your thigh muscles. This will push the knee down into extension. Typically, I tell my patients to hold this stretch for 10-15 minutes 3-4x a day (aim is 60 minutes total). Many doctors and therapists advocate for something called the prone hang. This can help restore extension, but I'm not a huge fan. This can be an uncomfortable and vulnerable position for a freshly post-op patient, as she is laying on her belly with both legs hanging off of the table, allowing gravity to push the knee straight. You can't control the pelvis in this position, and in many cases, restoring any hyperextension an athlete might have, is extremely difficult (Thanks to Lenny Macrina for this alternative!). Check out the pictures to see what I mean:

Prone Hang

Low-Load, Long Duration Stretching
After achieving knee extension (or hyperextension) passively, it's important to start using this range of motion actively to "lock in the gains." Many therapists and surgeons believe that once a patient can lift her leg into the air with a straight knee (or perform a straight leg raise without quadriceps lag), she can start walking without a brace, as the knee is much less likely to buckle. Many surgeons on the West Coast and in Europe don't even advocate using a brace, but I'll save that conversation for a different day. If you are intrigued – you can check out what the literature says about postoperative bracing here, here, and here.
Once an athlete can tolerate weight-bearing, she should focus on regaining single-leg balance and continue to work on quadriceps activation and strengthening. Some of my favorite ways to improve knee extension in weight-bearing are by retro walking on a treadmill or stepping backward over cones. When walking backward, you strike the ground with your toes and rock through your heel, creating an extension moment at the knee that can allow momentum to assist in actively straightening the knee. Check out the video below to see what I mean:
Retro-Walking on Treadmill
Knee Flexion Range-of-Motion
I know this is the part that many, if not most, ACL patients dread. Though somewhat painful, loss of knee flexion is much less common than loss of knee extension. While that statement likely won't provide you with a ton of comfort, know that there are a number of ways to ensure you regain all of your range of motion back after surgery. Heel slides, wall slides, or prone knee flexion with overpressure are all ways patients can practice bending their knee at home. Check out the pictures below:
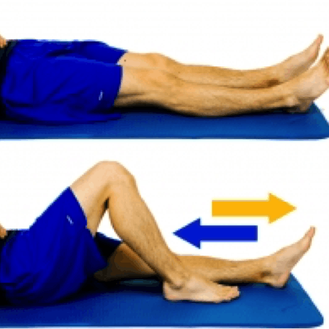
heel slides

wall slides

Prone Knee Flexion with Strap
As a clinician, I know that there are a number of positions and techniques that patients tolerate well, as well as a few that patients do not particularly enjoy. Physical therapists will either bend your knee with you laying on your back, your belly, or sitting at the edge of a table. As a former patient, I can say that the seated position is usually the most comfortable when ranging the knee. Sitting at the table's edge allows gravity to gently distract the tibia (shin bone) from the femur (thigh bone), providing a transient sense of pain relief. Furthermore, having a patient lay on her back or belly can make her feel uncomfortable, as the therapist towers above cranking her knee into flexion. The tibia can also sag posteriorly in these positions, resulting in impingement-like anterior knee pain. That's no bueno.
Many physical therapists aim to hit approximately 90 degrees of flexion by the end of the first week, with a full range of motion (125+ degrees) achieved by weeks four to six. Once a patient is weight-bearing, she can start to perform other exercises that reinforce knee flexion like mini squats or, eventually, lunges.

Less Comfortable

more comfortable
While I know that many of these details may seem daunting to the sidelined athlete, it is important to remember to control the controllables. Make sure you find a great physical therapist and start rehabilitation relatively soon after your surgery. This ensures that you are given the appropriate exercises, stretches, and manual therapy to promote the best possible recovery. Six or nine months may seem like a long time now, but when it comes to early ACL rehabilitation, I think Earl Nightingale said it best: "Don't let the fear of the time it will take to accomplish something stand in the way of your doing it. The time will pass anyway; we might just as well put that passing time to the best possible use."
Are you looking for other ways to manage your injury? Our therapists at Move Strong Physical Therapy can help. Get started here!
References:
- Sonnery-Cottet B, Saithna A, Quelard B, et al. Arthrogenic muscle inhibition after ACL reconstruction: a scoping review of the efficacy of interventions. Br J Sports Med. Published Online First: 07 September 2018.
- Lowe WR, Warth RJ, Davis EP, Bailey L. Functional bracing after anterior cruciate ligament reconstruction: A systematic review. J Am Acad Orthop Surg. 2017;25:239–49.
- Kruse LM, et al. Rehabilitation after anterior cruciate ligament reconstruction: a systematic review. J Bone Joint Surg Am. 2012 Oct 3;94(19):1737-48.
- Wright RW, et al. Bracing after ACL reconstruction: a systematic review. Clin Orthop Relat Res. 2007 Feb;455:162-8.
- Cooper R, Hughes M. Melbourne ACL rehabilitation guide. https://www.premax.co/us/all/acl-rehab-protocol. Published 2018.
- Macrina L. Three ways to avoid loss of motion after ACL reconstruction. https://championptandperformance.com/3-ways-avoid-loss-motion-acl-reconstruction/. Published October 2014.
Andrew MillettMarch 3, 2021
